A Case of Non-Union of Lateral Condyle of Humerus in Paediatric Age-treatment with Milch Osteotomy.
Singh Saurabh1, K Vinay1, Singh Ashutosh K1
1Assistant Professor, Department of Orthopedics, Institute of Medical Sciences, BHU, Varanasi.
2Senior Resident, Department of Orthopedics,Maulana Azad Medical College,New Delhi.
3Assistant Professor, Department of Orthopedics, Mayo Institute of Medical Sciences,Barabanki,India .
Address of Correspondence
Dr. A K Singh
C 1/157,Vishesh Khand,Gomti Nagar, Lucknow,Uttar Pradesh Pincode- 226010, India.
Email: ashu.ortho@gmail.com
Abstract
Objective: This study introduces a prospective comparative study to evaluate the effectiveness of implants of different design (titanium elastic intramedullary nail versus anatomical precontoured dynamic compression plate) in displaced midshaft clavicular fractures.
Methods: Seventy patients between 18 and 65 years of age were included in this study. They were randomized in two groups to be treated with either elastic intramedullary nail (EIN) or plate. Clinical and radiological assessments were performed at 1st, 3rd, 6th and 12th months postoperatively. Outcomes and complications of both the groups in 12 month follow-up time were compared.
Results: Length of incision, operation time, blood loss and duration of hospital stay was significantly less for EIN group. ASES and Constant Shoulder scores were significantly higher (p<0.05) in plating group than EIN group for first 3 months but there was no significant difference found between the two groups regarding functional and radiological outcome at 12 month follow up. Significantly higher rates of refracture after implant removal (p=0.045) in plating group was observed. Infection and revision surgery rate was also higher in plate group but this difference was insignificant (p>0.05).
Conclusions: EIN is a safe, minimally invasive surgical technique with lower complication rate, faster return to daily activities, excellent cosmetic and comparable functional results and can be used as an equally effective alternative of plate fixation in displaced midshaft clavicle fractures.
Key Words: displaced mid shaft clavicle fractures, elastic intramedullary nailing, anatomical precontoured plating.
Introduction
Fractures of the clavicle account for 2.6 to 4 % of all adult fractures, 35 % of all injuries to the shoulder girdle and 69-82% of these fractures occur in the middle-third [1]. Displacement occurs in about 73% of all midshaft clavicle fractures [2]. The average age of patients sustaining a midshaft clavicular fracture is 33 years, 70 % of the patients is male [3]. A fall or a direct blow to the shoulder, giving an axial compressive force on the clavicle, is the most common trauma mechanism of injury for any clavicular fracture [4,5]. Displaced midshaft fractures have traditionally been treated non-operatively because of early reports suggesting that clavicular non-unions are very rare and clavicular mal-union being of radiographic interest only, without clinical importance [6,7]. However, recent studies have found higher rates of delayed union, nonunion, shoulder pain, and shoulder weakness and residual pain with non-operative treatment [8]. The indications for surgery include the need for earlier functional mobilization in the patient with an isolated injury in addition to open fractures, floating shoulders and patients with polytrauma [9]. For operative treatment, the available methods of fixation are fixation with Kirschner wires, pins (Rush pin, Knowles pin, Rockwood pin), plates with screws and external fixation [10,11,12 ].
This prospective comparative study was designed to compare outcomes and complications of titanium elastic intranedullary nailing and anatomically precontoured plating in displaced midshaft clavicular fractures .

Methods
We conducted a prospective comparative study to compare outcomes and complications of closed displaced midshaft clavicular fractures treated with precontoured dynamic compression plate or with single titanium elastic intramedullary nail. This study was carried out at level 1 trauma centre, Institute of Medical Sciences, BHU and approved by the local ethical committee of Institute of Medical Sciences, BHU. All patients gave their informed consent. This was performed in accordance with the Ethical standards of the 1964 Declaration of Helsinki as revised in 2000. This study was powered to identify a clinically significant difference with 1−ß = 80%. The required sample size was calculated after setting the power to 80% and statistical significance at 5% level. Between July 2008 and June 2010, a total of 70 patients with closed displaced midshaft clavicular fractures were admitted in our hospital. In this study, these patients were randomized according to inclusion and exclusion criterias into two equal groups of 35 patients, to be treated surgically with either a 3.5 mm precontoured dynamic compression plate (plate group) or with a single titanium elastic intramedullary nail fixation (EIN group). The characteristics of the patients of both groups are shown in Table 1. Patients were randomized into two groups by the concealed envelope technique. The Robinson1 classification system is the most valuable in terms of choosing therapy, as well as being of prognostic value for midshaft clavicular fractures. In this study, we included angulated midshaft clavicle (type 2A2) fractures and displaced midshaft clavicle (type 2B1) fractures. Type 2B2 fractures were not included in this study because these fractures were segmental and markedly comminuted. According to Robinson classification system, 12 were type 2A2, 23 were 2B1 in plate group and in EIN group, 10 were type 2A2, 25 were type 2B1. Patients were followed for minimum 12 months postoperative time. In this study, 5 patients were lost to follow-up at 12 month postoperative visit. Only 3 of them could be contacted on telephone. All of them were asymptomatic and already had joined their duty. All these patients were within the working age group and they did not like to attend the clinic despite the offer of attendance fees and a certificate of attendance to facilitate taking time off work to attend the clinic. Remaining two patients could not be contacted because they had shifted to new place. Sixty five patients attended 12 months follow-up visit and we observed clinical and radiological parameters of the fracture along with complications in both groups.
Inclusion criterias:
• Age > 16 yrs and < 65 years of age
• duration < four weeks with no cortical bone contact
• shortening of over 10 mm and axial mal-alignment of over 30°.
• dislocation ,defined as at least one shaft width difference in height between the fracture parts, regardless of the reduction.
Patients were excluded if they had fractures with marked comminution, duration more than four weeks, open fractures, pre-existent morbidity of ipsilateral of the arm, shoulder or hand, presence of neurovascular injury and ipsilateral injuries
Operative technique
• Plate fixation:
Internal fixation was done according to AO principles. A transverse incision was made over the fracture site and dissection is carried out down to the fracture site, followed by careful subperiosteal dissection [13]. The fracture is reduced and held temporarily with bone clamps and plate positioned on the anterior superior surface of the clavicle (Figure 1A and 1B). Lots of different plates are being used now-a-days in clavicle fracture fixation. In this study, we have compared a precontoured 3.5 mm clavicular dynamic compression plate (Sharma pvt limited, Mumbai, India) with EIN. Additional interfragmentary lag screws were used in cases of oblique fractures. Drill stopper was used to avoid injury to neurovascular structures during drilling.
• EIN Fixation:
Elastic intramedullary nailing was done by technique described first by Jubel et al [14]. A small skin incision was made approximately 1 cm lateral to the sternoclavicular joint. Single elastic nail of different diameter varying from 2 to 3.5 mm, was used depending on the width of the bone. Closed reduction under image intensifier was done and provisionally fixed with two percutaneously pointed reduction clamps. If closed reduction failed, an additional small incision was made above the fracture site for direct manipulation of the main fragments then nail was introduced in the lateral fragment and the fracture was compressed. TEN was cut as short as possible at the medial end (figure 2A, 2B and 2C). In all cases, elastic nail of same make (Synthes, Switzerland) was used.
Postoperative management:
For both groups, patients received arm sling support for 2 weeks postoperatively and encouraged to start early mobilisation if pain permitted. Patients were encouraged to resume their normal daily activities after the 4th week when the pain was tolerated. Strenuous activities were allowed after 6th week postoperatively.

Operative time, length of incision, hospital stay, blood loss (calculated by the difference in the weights of the sponges pre- and postoperatively and the adding volumes of suction loss), pain visual analogue scale (0: none to 10:severe) on the first post-operative day were recorded for each patient. In follow-up visits, all patients were evaluated clinically at 1st, 3rd, 6th and 12th month to assess outcomes of fracture fixation in both groups like fracture union time, union rate, shoulder and arm function. Shoulder function was evaluated according to the American Shoulder and Elbow Surgeons (ASES) score and Constant Score,(both are the 100-point scoring system) [15]. These scoring systems combine assessments of subjective symptoms and objective findings. In Constant Scoring system, the overall grading is excellent if the total score ranges from 90 to 100, good for 80–89, fair for 70–79, and poor if the scores are 69 or less.
Complications were recorded and compared between both groups. Non-union was defined as an unsuccessful healing of the bone after six months, clinically manifesting as pain at fracture site and radiologically as a visible gap between the fracture parts. Deep infection was defined as infection requiring implant removal. Refracture was defined as a fracture of the clavicle with- in 3 months of implant removal without any history of retrauma.
Statistical analysis
The student’s t-test was used to analyze the difference of mean for different parameters. Mean, standard deviation and standard error of mean for the variables were also calculated. The test was referenced for two-tailed p-value and 95% confidence interval was constructed around sensitivity proportion using normal approximation method. Statistical analyses were performed using SPSS software. A value of <0.05 was considered statistically significant.
Results
In this study, during a 2-year period from July 2008 to June 2010, 70 patients with displaced midshaft clavicle fractures were included as per inclusion criteria and underwent surgical fixation. Only 65 out of 70 patients could be followed upto 1 year, 32 patients underwent open reduction and internal fixation with precontoured dynamic compression plate (Plating Group) and 33 patients underwent closed or open reduction (done when closed reduction failed) and antegrade titanium elastin nailing (EIN Group). In the EIN group, closed fracture reduction and internal fixation was done in 14 cases (42.42 %), and open reduction was required in the remaining 18 patients (56.25%). The average age in the plating group was 24.6 (range, 18–64) years and in the elastic nailing group was 26.4 (range, 20–62) years. Gender proportions in the two groups were considered to be similar (p=0.64). Both groups showed no statistical difference in term of age (p = 0.82), gender (p = 0.64), the time from injury to operation (p = 0.62). Surgery was performed with- in 7 days (range,1-7days) of injury time in all cases. Demographic profile of both groups is shown in Table 1.
There was significant difference in both groups (less in EIN group) regarding mean operative time (p=0.041), blood loss (p=0.004) and length of hospital stay (p=0.032) as shown in Table 2. The average bone union time was shorter in the EIN group (6.1 months ± 1.8 ; range 2.5–8 months) than in the plating group (7.4 months ± 2.7 ; range 3–11 months) but this difference was insignificant(p = 0.68).
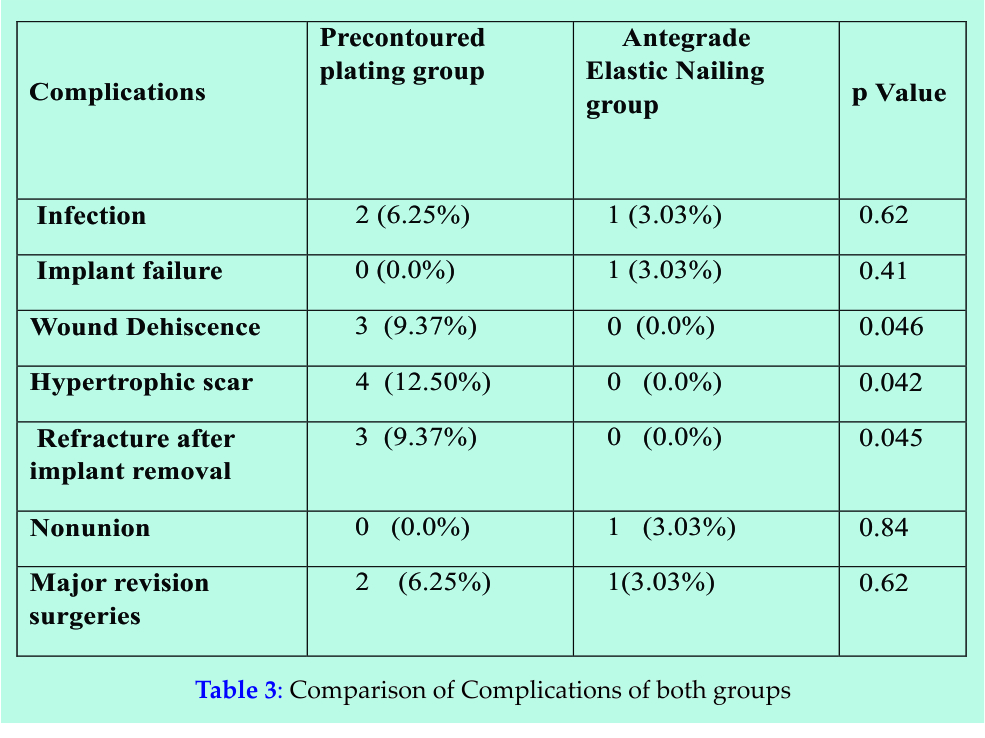
Two cases in plate group and one case in EIN group developed superficial infection (p=0.62) but infection was controlled by oral antibiotics in all three cases. There was no deep infection in any case of both groups. Nonunion occurred in one case in EIN group while in plating group, all fractures united (p=0.84) (Table 3).
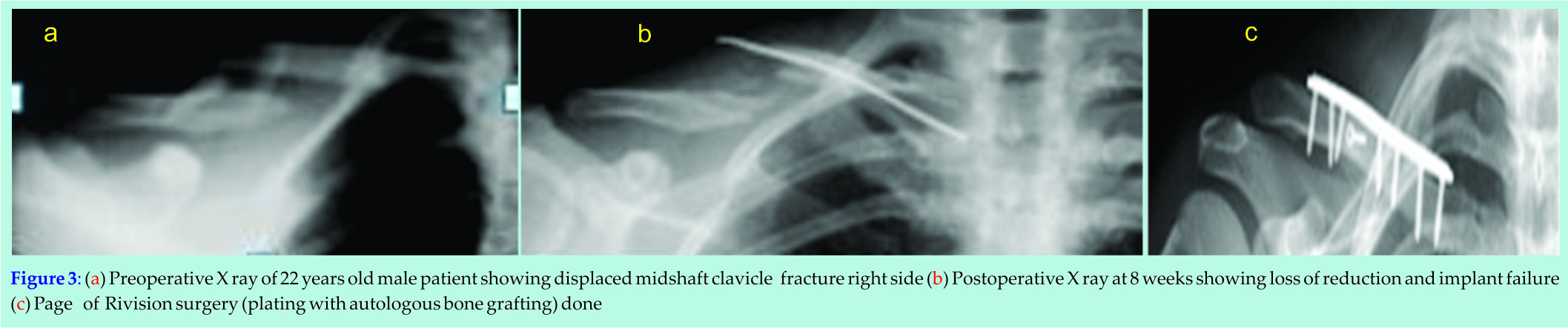
No implant failure occurred in the plate group while one implant failure (figure 3A and 3B) was seen in the EIN group (3.03 %) (p= 0.41) which occurred within three months of the primary surgical procedure. Open reduction and plating with autogenous bone grafting in this case resulted in bone union finally (figure 3C). Three refractures (9.37 %) were observed in the plate group after removal of the implant while no such complication seen in the EIN group (p = 0.045). All refractures occurred within 1 month after plate removal. Out of these three refractures, one was treated conservatively and plating was done in two cases, leading to uneventful healing. Hypertrophic scar formation was observed in 4 cases of plating group, none in EIN group (p=0.042), wound dehiscence seen in 3 cases of plating group while none in EIN group(p=0.046).
In the EIN group, elastic nails were removed in all cases. In the plate group, 20 patients (total of 32 patients) underwent implant removal. In the EIN group the nail was removed at an average time of 6.2 months (range, 4–7 months). Plates were removed at an average time of 15.4 months (range, 11-20 months) (p < 0.05).
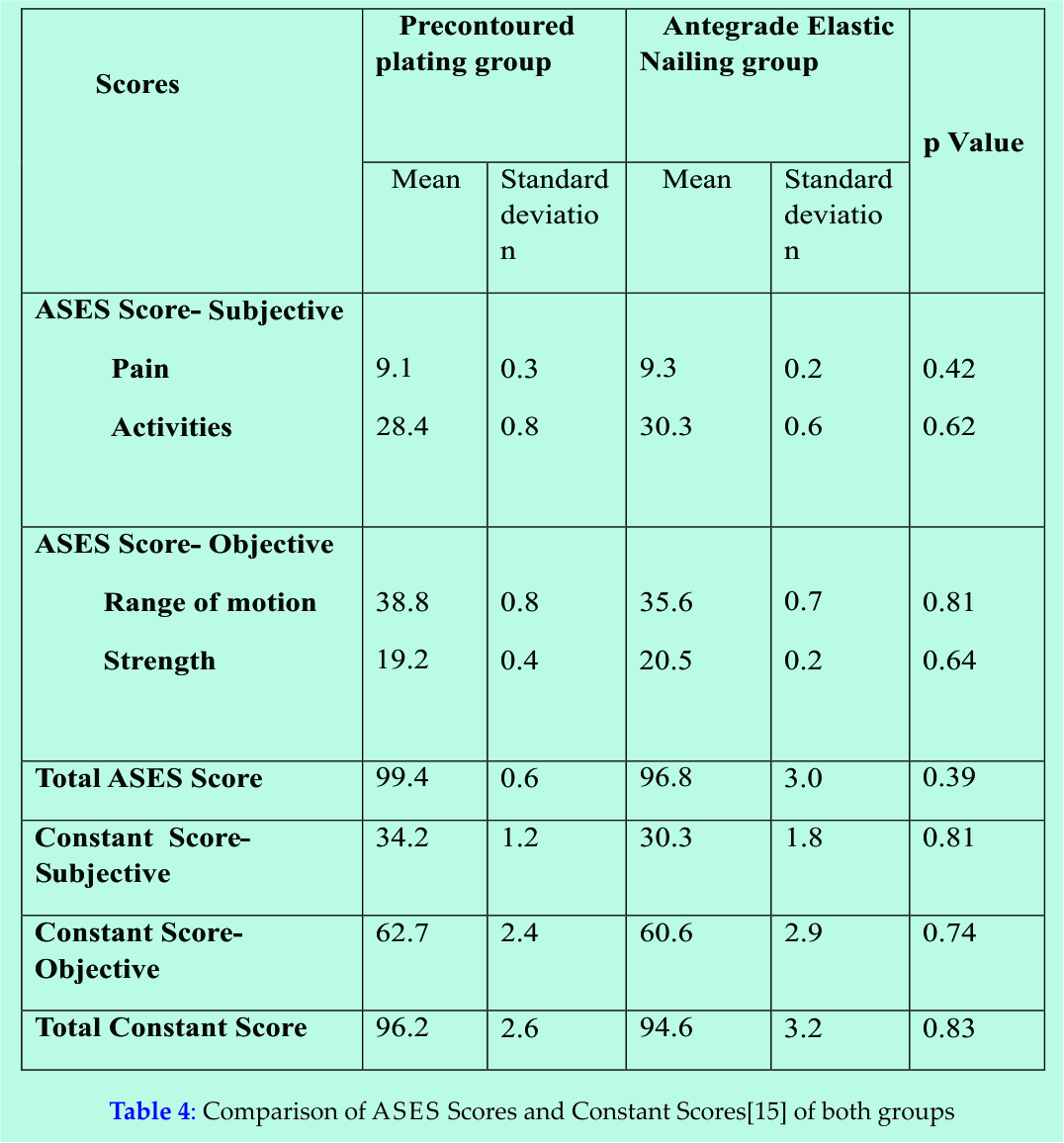
ASES and Constant Shoulder scores were assessed at every follow-up visit and 1 month postoperative follow-up visit showed significant higher Constant scores of 74.1 ± 8.2 in the plating group than in the EIN group [60.1 ± 10.2] (p=0.04). Final scores at 12 month follow up visit showed no significant difference between two groups as shown in Table 4(p>0.05).
Discussion
The best treatment strategy for displaced midshaft clavicle fractures remains a topic of debate. Conservative management of these fractures results in approximately 5% nonunion rate. 4 While non-operative management remains the mainstay of treatment for most midshaft clavicle fractures, the indications for surgery may be expanding. Recent studies have showed a poorer outcome in cases of displaced midshaft clavicle fractures that were treated nonoperatively 8 [16,17]. in comparison to surgically treated patients. 14,18,19. Three types of fixation are available for middle-third clavicle fractures: intramedullary devices, plates, and external fixators. Intramedullary fixation can be done by smooth or threaded K- wires, Steinman pins, Knowles pins, Hagie pins, Rush pins or cannulated screws [20,21,22]. Plate fixation can be done with 3.5mm dynamic compression plate (DCP), low-contact dynamic compression plates, reconstruction plates or locking compression plates with at least three screws (six cortices) in both the medial and lateral fragment each and an interfragmentary lag screw whenever the fracture pattern allows it. Plating of acute clavicle fractures is advocated as the preferred fixation method by many authors[23,24]. Biomechanically, plate fixation is superior to intramedullary fixation because it better resists the bending and torsional forces that occur during elevation of the upper extremity above shoulder level [25]. Patients treated with plate fixation can be allowed full range of motion once their soft tissues have healed. Disadvantages of plate fixation include the necessity for increased exposure and soft-tissue stripping, increased risk of damage to the supraclavicular nerve, slightly higher infection rates, and the risk of refracture after plate removal. 7 Currently, Open reduction and internal fixation with a 3.5 mm dynamic compression plate [26,27] is the standard method; however, intramedullary fixation [14,28]. is a equaqlly effective alternative. In this study ,both methods of fixation were compared in terms of outcomes and complications.
In our study, functional Shoulder scores were significantly higher for plating group than EIN group in first 12 weeks but at 12 month follow up visit, there was no significant difference observed between two groups in terms of Shoulder scores. In this study, in plating group, rates of refracture (9.37 %), major revision surgery (6.25%) and implant failure (3.03 %) were comparable to other studies. The Canadian Orthopaedic Trauma Society reported one (1.6 %) case of early mechanical failure.5 Bostman et al. studied 103 patients treated with open reduction and internal fixation using plates; among those patients, 43% had complications; 15%, major complications; and 14% required re-operation and implant failure rate of 14.6 %. 29Chen et al. reported 7.1 % implant failure. 30Liu et al. compared titanium elastic nail and reconstruction plate fixation in displaced midshaft clavicle fractures and found no significant difference between intramedullary- and plate fixation after 18 months in terms of functional outcome (DASH score p = 0.42, Constant score p = 0.17) and complications. They reported an implant failure rate of 8.5 %. Reason behind this higher refracture rate after implant removal in plating group is that plate fixation provides a rigid fixation leading to primary bone healing that’s why after plate removal , mechanical strength of healed fracture site is reduced explaining higher refracture rates. Along with this, screw holes may act as stress risers leading to refractures. Secondary bone healing occurs in cases of fractures treated with EINs so refracture rate after removal of the implant is less in these cases. For plate fixation, a larger incision is required leading to a higher risk of infection and lesser cosmetic satisfaction but in our study no significant differences in infection rates between the two groups were found
Ferran et al. 32 compared Rockwood pin fixation (17 cases) and low contact dynamic compression(LCDCP) plate (15 cases) in displaced midshaft clavicle fractures and found no significant difference after 12 months in functional outcome (Constant score p = 0.37). Complications occurred in 12% of the intramedullary fixation group and in 40% of plate fixation group. Bohme et al. 33 and Thyagarajan34 et al. reported same conclusions in their study comparing plating, intranedullary fixation and conservative treatment in displaced midshaft clavicle fractures.
In a retrospective study done by Wu et al. , comparison between plating and intramedullary nailing for the treatment of clavicular nonunion35 showed an 18.2% nonunion rate with plating compared with 11.1% for nailing, the difference being attributed to the nail’s resistance to compressive stresses. The authors concluded that plating provides better rotational stability. Several other studies have found intramedullary fixation to be equally effective as plating, especially for the treatment of nonunion. 36,37 Refracture after implant removal and major revision surgery just tended to prevail more often after plate fixation while implant failure was more common in EIN group. Major revision procedures were done in EIN group due to implant failure while in plating group due to refracture after implant removal. The minor revision surgeries were common in EIN group for problems like medial protrusion causing irritation or skin perforation. Implant removal in plating group needed another surgery done under general anesthesia, and large-sized incision was made, while in EIN group, nail was removed as an outdoor procedure under local anesthesia and a small incision over the tip of the nail was made. This was another advantage of intramedullary flexible nailing over plating.
Our study has limitations. This was a small prospective study. A randomized controlled trial with a larger sample size is required in future to confirm the outcome achieved in our study by the two groups of patients treated for displaced and shortened mid-clavicle fractures. But still we can conclude from our study that both, precontoured plating and intramedullary flexible nailing are equally effective alternatives for surgical fixation of displaced mid shaft clavicular fractures. Antegrade flexible intramedullary nailing technique have advantages like less soft tissue injury, shorter operating time and hospital stay, less blood loss, cosmetically more satisfaction and minor surgery needed to remove implant. EIN is a safe minimally invasive surgical technique with lower complication rate, faster return to daily activities, excellent cosmetic and comparable functional results, which can be regard as an alternative to plate fixation of displaced mid-shaft clavicular fractures.
References
1. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br. 1998; 80:476–484.
2. Khan LA, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg (Am) 2009; 91:447–60.
3. Pearson AM, Tosteson ANA, Koval KJ, McKee MD, Cantu RV, Bell JE et al. Is Surgery for Displaced, Midshaft Clavicle Fractures in Adults Cost-Effective? Results Based on a Multicenter Randomized, Controlled Trial. Journal of Orthopaedic Trauma. 2010; 24:426–433.
4. Nowak J, Mallmin H, Larsson S. The etiology and epidemiology of clavicular fractures. A prospective study during a two-year period in Uppsala, Sweden. Injury. 2000; 31:353–358.
5. Stanley D, Trowbridge EA, Norris SH. The mechanism of clavicular fracture. A clinical and biomechanical analysis. J Bone Joint Surg Br. 1988; 70:461–464.
6. Neer CS. Nonunion of the clavicle. J Am Med Assoc. 1960; 172:1006–101.
7. Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007; 89:1–10.
8. Hill JM, McGuire MH, Crosby LA. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br. 1997; 79:537–539.
9. Denard PJ, Koval KJ, Cantu RV, Weinstein JN. Management of midshaft clavicle fractures in adults. Am J Orthop. 2005; 34:527–536.
10. Lee YS, Lin CC, Huang CR, Chen CN, Liao WY. Operative treatment of midclavicular fractures in 62 elderly patients: Knowles pin versus plate. Orthopedics. 2007; 30(11):959–964.
11. Mudd CD, Quigley KJ, Gross LB (2011) Excessive complications of open intramedullary nailing of midshaft clavicle fractures with the Rockwood clavicle pin. Clin Orthop Relat Res 469(12):3364–3370.
12. Mueller M, Rangger C, Striepens N, Burger C. Minimally invasive intramedullary nailing of midshaft clavicular fractures using titanium elastic nails. J Trauma. 2008; 64(6):1528–1534.
13. Poigenfürst J, Rappold G, Fisher W. Plating of fresh clavicular fractures: results of 122 operations. Injury. 1992; 23(4):237–241.
14. Jubel A, Andermahr J, Schiffer G, Tsironis K, Rehm KE (2003) Elastic stable intramedullary nailing of midclavicular fractures with a titanium nail. Clin Orthop Relat Res 408:279–285.
15. Constant CR, Murley AG. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987;214:160–164
16. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE (2004). Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg 86-A:1359–1365.
17. Wild LM, Potter J (2006) Deficits following nonoperative treatment of displaced midshaft clavicular fractures. J Bone Joint Surg 88-A:35-40.
18. Ali KM, Lucas HK. Plating of fractures of the middle third of the clavicle. Injury. 1978; 9(4):263–267.
19. Jeray K. Acute midshaft clavicular fracture. J Am Acad Orthop Surg. 2007;15:239–248.
20. Kyle RF, Schmidt AH. Open Reduction and Internal Fixation of Fractures and Nonunions. In: Thompson RC, ed. The Shoulder. New York: Raven Press, 1995;183
21. Neviaser RJ, Neviaser JS, Neviaser TJ. A Simple Technique for Internal Fixation of the Clavicle: A Long Term Evaluation. Clin Orthop 1975; 109:103.
22. Ngarmukos C, Parkpian V, Patradul A. Fixation of Fractures of the Midshaft of the Clavicle with Kirschner Wires: Results in 108 Patients. J Bone Joint Surg 1998;80B:106
23. Mullaji AB, Jupiter JB. Low-Contact Dynamic Compression Plating of the Clavicle. Injury 1994; 25:41.
24. Ring D, Jupiter JB, Miller ME, Ada JR. Injuries to the Shoulder Girdle: Part II. Fractures of the Clavicle. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, eds. Skeletal Trauma, Vol 2. Philadelphia: WB Saunders, 1998;1670.
25. Golish SR, Oliviero JA, Francke EI, Miller MD. A biomechanical study of plate versus intramedullary devices for midshaft clavicle fixation. J Orthop Surg Res. 2008;16(3):28.
26. Kloen P, Sorkin AT, Rubel IF, Helfet DL. Anteroinferior plating of midshaft clavicular nonunions. J Orthop Trauma. 2002;16:425–430.
27. Schwarz N, Hocker K. Osteosynthesis of irreducible fractures of the clavicle with 2.7-mm ASIF plates. J Trauma. 1992;33:179–183.
28. Rehm KE, Andermahr J, Jubel A Intramedullary nailing of midclavicular fractures with an elastic titanium nail. Eur J Traum Emerg Surg2005: 31(4)
29. Böstman O, Manninen M, Pihlajamäki H. Complications of plate fixation in fresh displaced midclavicular fractures. J Trauma. 1997; 43:778–783.
30. Chen YF, Wei HF, Zhang C, Zeng BF, Zhang CQ, Xue JF et al (2012) Retrospective comparison of titanium elastic nail (TEN) and reconstruction plate repair of displaced midshaft clavicular fractures. J Shoulder Elbow Surg 21:495–501.
31. Liu HH, Chang CH, Chia WT, Chen CH, Tarng YW, Wong CY. Comparison of plates versus intramedullary nails for fixation of displaced midshaft clavicular fractures. J Trauma. 2010; 69(6):E82–E87.
32. Ferran NA, Hodgson P, Vannet N, Williams R, Evans RO. Locked intramedullary fixation vs plating for displaced and shortened mid-shaft clavicle fractures: a randomized clinical trial. J Shoulder Elbow Surg. 2010;19:783–789.
33. Böhme J, Bonk A, Bacher GO, Wilharm A, Hoffmann R, Josten C. Current treatment concepts for mid-shaft fractures of the clavicle – results of a prospective multicentre study. Z Orthop Unfall.2010;149(1):68–76.
34. Thyagarajan DS, Day M, Dent C, Williams R, Evans R. Treatment of mid-shaft clavicle fractures: a comparative study. Int J Shoulder Surg. 2009; 3(2):23–27.
35. Wu CC, Shih CH, Chen WJ, Tai CL. Treatment of clavicular aseptic nonunion: comparison of plating and intramedullary nailing techniques. J Trauma. 1998; 45:512–516.
36. Capicotto PN, Heiple KG, Wilbur JH. Midshaft clavicle nonunions treated with intramedullary Steinman pin fixation and onlay bone graft. J Orthop Trauma. 1994;8:88.
37. Enneking TJ, Hartlief MT, Fontijne WP. Rush pin fixation for midshaft clavicular nonunions: good results in 13/14 cases. Acta Orthop Scand. 1999;70:514–516 .
| How to Cite: Saurabh S, Vinay K, Singh AK. Surgical Fixation of Displaced Mid Shaft Clavicle Fractures: Elastic Intramedullary Nailing Versus Anatomical Precontoured Plating. Journal of Orthopaedic and Rehabilitation 2015 Jult-Sep; 1(2): 6-12 |
[Full Text HTML] [Full Text PDF]